Bispecific antibodies have emerged as a promising class of immunotherapies in oncology, offering innovative treatment options for various cancers. These engineered antibodies are designed to simultaneously bind 2 different targets, enhancing the immune system’s ability to recognize and eliminate cancer cells.1 Notable examples include blinatumomab for acute lymphoblastic leukemia and teclistamab for multiple myeloma.2,3
Despite their therapeutic potential, the adoption and utilization of bispecific antibodies exhibit significant disparities, particularly between urban and rural healthcare settings.4 In urban areas, where advanced medical infrastructure and specialized oncology centers are more prevalent, the use of bispecific antibodies is more concentrated.4 Conversely, rural regions often face challenges in accessing these therapies, leading to a concentration of their use in cities.4
Several factors contribute to the limited use of bispecific antibodies in rural areas. First, infrastructure limitations play a significant role, as administering bispecific antibodies requires specialized medical expertise and organization, including inpatient oncology services capable of monitoring patients during the initial dosing phases.4 Many rural clinics lack the necessary facilities and trained personnel to safely administer these therapies.4 Financial constraints also pose a major barrier, as the high cost of bispecific antibody treatments creates a significant financial burden for rural healthcare facilities, which may lack the resources to invest in these advanced therapies.5 This financial strain further limits the availability of such treatments in rural settings.5 Additionally, the geographic distribution of clinical trials for these therapies exacerbates access issues.6 A study found that 34% of US states had no open clinical trials for chimeric antigen receptor T cells and bispecific antibodies.6 States with higher percentages of Black residents, who face a higher incidence of multiple myeloma, were particularly affected, suggesting that the current distribution of clinical trials contributes to disparities in access to advanced therapies.6
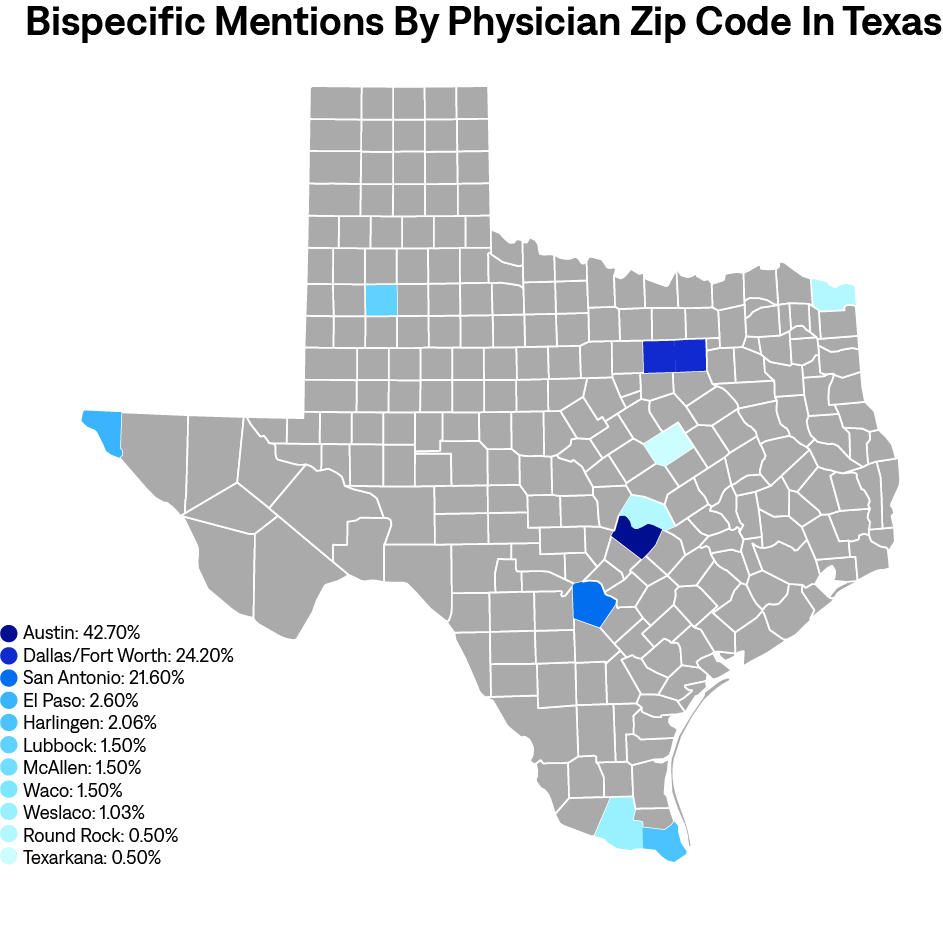
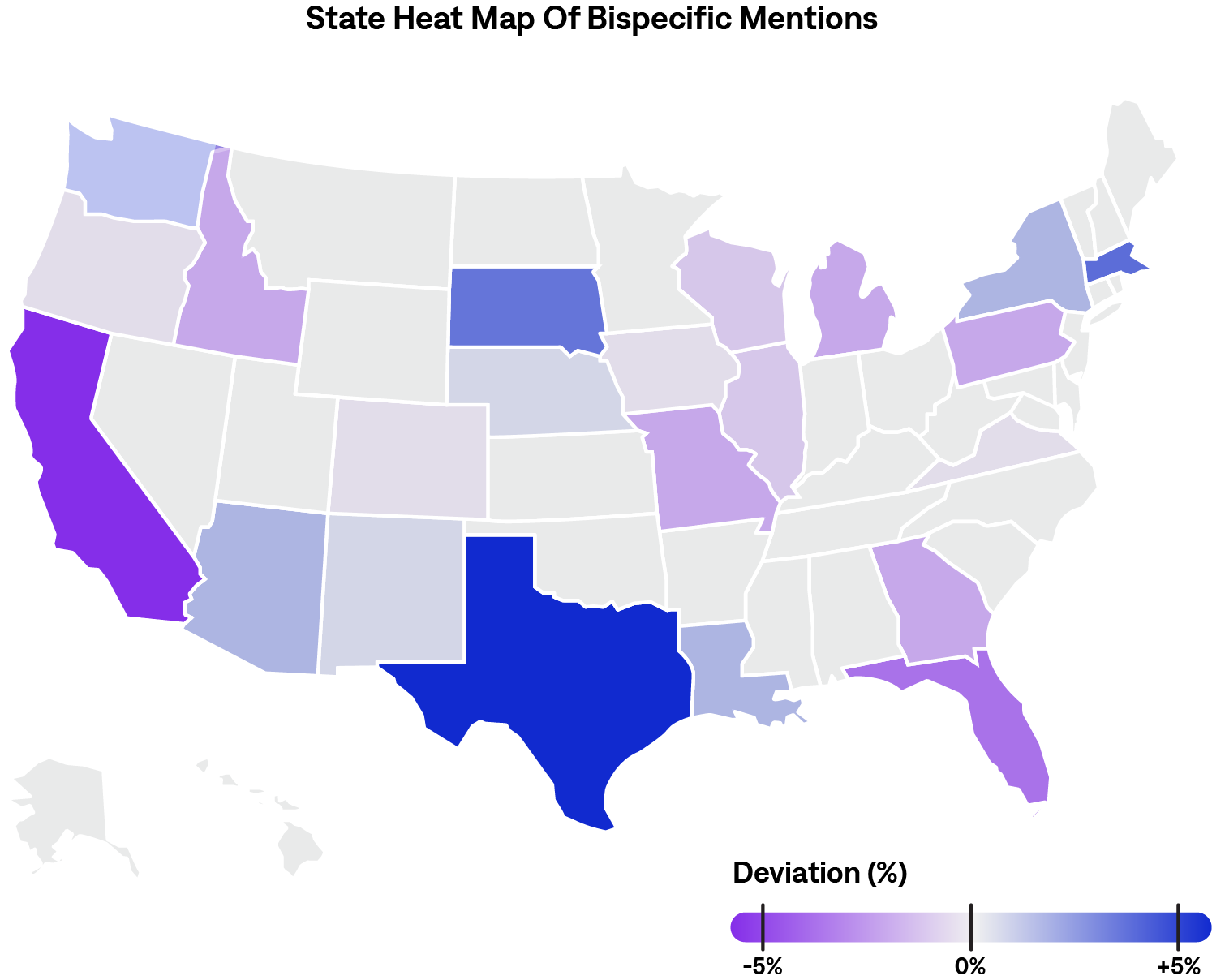
Real-world data can be used to further understand trends in the use of bispecific antibodies and to better recognize where there may be areas of inequity. AnswerY™ is a proprietary database and platform composed of US-based transcribed physician notes which uses natural language processing to extract structured results from detailed patient visit records. This database, which consists of over 80 million records, allows users to gain actionable insights from real-world data that goes beyond claims and ICD10 codes. AnswerY was searched for any mention of “bispecific antibody” across any indication. 864 patients matching 1819 records met these criteria. Figure 1 shows the geographic distribution of bispecific mentions in the United States, with red states demonstrating higher counts than would be expected compared with the overall database. An analysis of Texas revealed that most patients with records mentioning “bispecific antibodies” were treated by physicians in the zip codes of larger cities; 42.7% Austin, 24.2% Dallas/Fort Worth, and 21.6% San Antonio (Figure 2). Although there were some results in more rural areas of Texas, the raw records, in some cases, provided further insight into why this was the case. For example, when looking into the record of a patient-physician visit in Texarkana, it was found that this physician was a pain specialist and was seeing a patient who was on a bispecific antibody; however, this particular physician was not their treating oncologist. This may suggest that, although there was 1 record in Texarkana, this patient may still be traveling far distances to receive treatment. Findings from this real-world database support the need for increased efforts to increase adoption and utilization of bispecific antibodies in rural areas.
Recognizing these challenges, several initiatives are working to improve the accessibility of bispecific antibody therapies in rural areas. One such initiative has been spearheaded by the Association of Community Cancer Centers, which launched educational programs to prepare cancer care teams for the successful incorporation of these therapies into their practice.7 Additionally, organizations are sharing operational insights to assist in the delivery of bispecific antibodies, equipping care teams in community and rural cancer programs with the knowledge needed to administer these treatments effectively.4 Collaboration between academic centers and community practices is also crucial to improve access to bispecific antibodies. With a successful partnership, community oncologists can refer patients to academic centers for their initial treatment with the following cycles being managed by their local practices, while helping mitigate costs for community centers.4,5 Moreover, pharmaceutical companies and patient advocacy groups are offering financial support resources to help alleviate the financial burden on rural healthcare facilities, ensuring the availability of bispecific antibody therapies in community clinics and oncology centers.5
While bispecific antibodies represent a significant advancement in cancer treatment, their utilization is currently more concentrated in urban areas due to infrastructure, financial, and geographic challenges, which was supported by real-world data from the AnswerY database. Addressing these disparities is crucial to ensure equitable access to these therapies for all patients, regardless of geographic location. Ongoing efforts to integrate bispecific antibodies into community oncology practices and provide financial support are steps in the right direction toward eliminating these disparities.
Dig Deeper: Explore AnswerY, our HIPAA-complaint database of patient-provider conversations.